Suicide Prevention by Limiting Access to Methods a Review of Theory and Practice

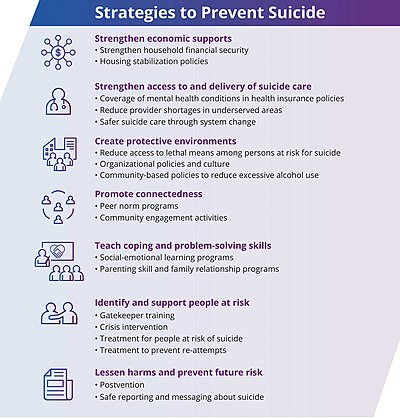
Suicide prevention measures suggested by the CDC[1]
Suicide prevention is a collection of efforts to reduce the risk of suicide.[ii] Suicide is frequently preventable,[three] and the efforts to forestall it may occur at the individual, relationship, customs, and society level.[2] Suicide is a serious public wellness trouble that can take long-lasting effects on individuals, families, and communities. Preventing suicide requires strategies at all levels of society. This includes prevention and protective strategies for individuals, families, and communities. Suicide tin exist prevented past learning the warning signs, promoting prevention and resilience, and a committing to social change. [4]
Beyond directly interventions to end an impending suicide, methods may include:
- treating mental illness
- improving coping strategies of people who are at risk
- reducing risk factors for suicide, such as poverty and social vulnerability
- giving people hope for a amend life after electric current problems are resolved
- calling a suicide hotline number
General efforts include measures within the realms of medicine, mental health, and public wellness. Because protective factors[5] such as social back up and social engagement—besides as environmental gamble factors such as admission to lethal means— play a function in suicide, suicide is not solely a medical or mental-health issue.[six]
Interventions [edit]
Lethal-means reduction [edit]

Means reduction — reducing the odds that a suicide attempter volition use highly lethal means — is an important component of suicide prevention.[seven] This practice is also called "means restriction". It has been demonstrated that restricting lethal means tin can aid reduce suicide rates, as delaying action until the want to die has passed.[8] In general, strong evidence supports the effectiveness of means brake in preventing suicides.[ix] [ten] [11] [12] There is as well potent evidence that restricted admission at and so-chosen suicide hotspots, such equally bridges and cliffs, reduces suicides, whereas other interventions such as placing signs or increasing surveillance at these sites appears less constructive.[13]
I of the most famous historical examples of means reduction is that of coal gas in the United Kingdom. Until the 1950s, the nearly common means of suicide in the UK was poisoning by gas inhalation. In 1958, natural gas (virtually gratis of carbon monoxide) was introduced, and over the next decade, comprised over l% of gas used. Equally carbon monoxide in gas decreased, suicides also decreased. The decrease was driven entirely by dramatic decreases in the number of suicides by carbon monoxide poisoning.[14] [15] A 2020 Cochrane review on means restrictions for jumping found tentative evidence of reductions in frequency.[16]
In the United States, firearm access is associated with increased suicide completion.[17] About 85% of suicide attempts with a gun outcome in death, while most other widely used suicide attempt methods result in death less than 5% of the fourth dimension.[18] [xix] Matthew Miller, M.D., Sc.D. conducted inquiry comparing the number of suicides in states with the highest rates of gun ownership, to the number of suicides in states with the lowest rates of gun ownership. He establish that men were iii.7 times more than likely to die past firearm suicide and women were 7.9 times more than likely to die by firearm suicide living in states with high rates of gun buying. There was no divergence in non-firearm suicides.[20] Although restrictions on access to firearms have reduced firearm suicide rates in other countries, such restrictions are hard in the U.s. because the 2nd Amendment to the United States Constitution limits restrictions on weapons.[21]
Crises hotline [edit]


As a suicide prevention initiative, signs on the Golden Gate Bridge promote special telephones that connect to a crisis hotline, as well equally a 24/7 crisis text line.
Crisis hotlines connect a person in distress to either a volunteer or staff fellow member.[3] This may occur via telephone, online conversation, or in person.[three] Even though crisis hotlines are common, they have not been well studied.[22] [23] One report institute a subtract in psychological pain, hopelessness, and want to die from the first of the call through the next few weeks; however, the want to dice did non decrease long term.[3]
[edit]
In the United states of america, the 2012 National Strategy for Suicide Prevention promotes various specific suicide prevention efforts including:[24]
- Developing groups led by professionally trained individuals for wide-based back up for suicide prevention.
- Promoting community-based suicide prevention programs.
- Screening and reducing at-hazard behavior through psychological resilience programs that promotes optimism and connectedness.
- Education about suicide, including risk factors, alert signs, stigma related bug and the availability of aid through social campaigns.
- Increasing the proficiency of health and welfare services at responding to people in need. eastward.1000., sponsored training for helping professionals, increased access to community linkages, employing crisis counseling organizations.
- Reducing domestic violence and substance abuse through legal and empowerment means are long-term strategies.
- Reducing access to convenient means of suicide and methods of self-harm. due east.g., toxic substances, poisons, handguns.
- Reducing the quantity of dosages supplied in packages of non-prescription medicines due east.g., aspirin.
- School-based competency promoting and skill enhancing programs.
- Interventions and usage of ethical surveillance systems targeted at high-risk groups.
- Improving reporting and portrayals of negative behavior, suicidal behavior, mental affliction and substance abuse in the entertainment and news media.
- Research on protective factors & development of effective clinical and professional person practices.
Media guidelines [edit]
Recommendations around media reporting of suicide include not sensationalizing the event or attributing it to a unmarried cause.[3] It is also recommended that media messages include suicide prevention messages such as stories of promise and links to further resource.[3] [25] Particular care is recommended when the person who died is famous.[26] Specific details of the method or the location are not recommended.[26]
There is trivial bear witness, however, regarding the benefit of providing resources for those looking for assist and the evidence for media guidelines mostly is mixed at all-time.[27]
Tv shows and news media may also be able to help foreclose suicide by linking suicide with negative outcomes such as pain for the person who has attempted suicide and their survivors, conveying that the majority of people cull something other than suicide in lodge to solve their problems, avoiding mentioning suicide epidemics, and fugitive presenting authorities or sympathetic, ordinary people every bit spokespersons for the reasonableness of suicide.[28]
Medication [edit]
The medication lithium may be useful in certain situations to reduce the risk of suicide.[29] Specifically it is effective at lowering the risk of suicide in those with bipolar disorder and major depressive disorder.[29] [30] Some antidepressant medications may increase suicidal ideation in some patients under certain atmospheric condition.[31]
Counseling [edit]
There are multiple talk therapies that reduce suicidal thoughts and behaviors including dialectical behavior therapy (DBT).[32] [33] Cognitive behavior therapy for suicide prevention (CBT-SP) is a class of DBT adapted for adolescents at high risk for repeated suicide attempts.[34] [35] The brief intervention and contact technique developed by the Globe Health Organization also has shown benefit.[36]
The Earth Health Organization recommends "specific skills should be available in the instruction system to prevent bullying and violence in and effectually the schoolhouse".[37]
Coping planning [edit]
Coping planning is a strengths-based intervention that aims to come across the needs of people who ask for aid, including those experiencing suicidal ideation.[38] By addressing why someone asks for help, the take chances cess and direction stays on what the person needs, and the needs assessment focuses on the individual needs of each person.[39] [twoscore] The coping planning approach to suicide prevention draws on the health-focused theory of coping. Coping is normalized every bit a normal and universal man response to unpleasant emotions, and interventions are considered a change continuum of low intensity (due east.g., cocky-soothing) to high intensity support (eastward.thousand. professional help). Past planning for coping, it supports people who are distressed and provides a sense of belongingness and resilience in handling of illness.[41] [42] The proactive coping planning approach overcomes implications of ironic process theory.[43] The biopsychosocial[44] strategy of grooming people in good for you coping improves emotional regulation and decreases memories of unpleasant emotions.[45] A skilful coping planning strategically reduces the inattentional incomprehension for a person while developing resilience and regulation strengths.[41]
Strategies [edit]

A United states Army suicide prevention affiche
The traditional arroyo has been to place the run a risk factors that increase suicide or self-impairment, though meta-analysis studies suggest that suicide run a risk assessment might not be useful and recommend immediate hospitalization of the person with suicidal feelings as the good for you choice.[46] In 2001, the U.S. Department of Wellness and Human Services, published the National Strategy for Suicide Prevention, establishing a framework for suicide prevention in the U.South. The document, and its 2012 revision, calls for a public health arroyo to suicide prevention, focusing on identifying patterns of suicide and suicidal ideation throughout a grouping or population (every bit opposed to exploring the history and health conditions that could lead to suicide in a single private).[47] The power to recognize warning signs of suicide allows individuals who may be concerned almost someone they know to direct them to help.[48]
Suicide gesture and suicidal desire (a vague wish for death without whatsoever bodily intent to kill oneself) are potentially cocky-injurious behaviors that a person may utilise to attain some other ends, like to seek assistance, punish others, or to receive attention. This behavior has the potential to aid an private's capability for suicide and can exist considered as a suicide warning, when the person shows intent through verbal and behavioral signs.[49]
Specific strategies [edit]
Suicide prevention strategies focus on reducing the risk factors and intervening strategically to reduce the level of take a chance. Hazard and protective factors unique to the individual can exist assessed by a qualified mental health professional person.
Some of the specific strategies used to address are:
- Crisis intervention.
- Structured counseling and psychotherapy.
- Hospitalization for those with low adherence to collaboration for help and those who crave monitoring and secondary symptom treatment.
- Supportive therapy similar substance abuse treatment, Psychotropic medication, Family unit psychoeducation and Access to emergency telephone telephone call care with emergency rooms, suicide prevention hotlines, etc.
- Restricting access to lethality of suicide means through policies and laws.
- Creating and using crunch cards, an easy-to-read uncluttered carte that describes a list of activities one should follow in crisis until the positive behavior responses settles in the personality.
- Person-centered life skills grooming. due east.one thousand., Problem solving.
- Registering with support groups like Alcoholics Anonymous, Suicide Bereavement Back up Grouping, a religious grouping with period rituals, etc.
- Therapeutic recreational therapy that improves mood.
- Motivating cocky-care activities like physical exercises and meditative relaxation.
Psychotherapies that have shown well-nigh successful or testify based are dialectical behavior therapy (DBT), which has shown to be helpful in reducing suicide attempts and reducing hospitalizations for suicidal ideation[50] and cerebral behavioral therapy (CBT), which has shown to amend problem-solving and coping abilities.[51]
After a suicide [edit]
Postvention is for people affected by an individual'southward suicide. This intervention facilitates grieving, guides to reduce guilt, guides to reduce anxiety and depression, and helps to subtract the furnishings of trauma. Bereavement is ruled out and promoted for catharsis and supporting their adaptive capacities before intervening depression and any psychiatric disorders. Postvention is also provided to minimize the risk of imitative or copycat suicides, merely there is a lack of evidence based standard protocol. The general goal of the mental wellness practitioner is to decrease the likelihood of others identifying with the suicidal behavior of the deceased as a coping strategy in dealing with adversity.[52]
Adventure assessment [edit]

A photo analogy produced by the Defense force Media Agency on suicide prevention
Warning signs [edit]
Warning signs of suicide can permit individuals to straight people who may exist considering suicide to become assistance.[53]
Behaviors that may exist warning signs include:[54]
- Talking near wanting to die or wanting to kill themselves
- Suicidal ideation: thinking, talking, or writing about suicide, planning for suicide
- Substance abuse
- Feelings of purposelessness
- Anxiety, agitation, beingness unable to sleep, or sleeping all the time
- Feelings of existence trapped
- Feelings of hopelessness
- Social withdrawal
- Displaying extreme mood swings, suddenly changing from sad to very at-home or happy
- Recklessness or impulsiveness, taking risks that could lead to expiry, such as driving extremely fast
- Mood changes including depression
- Feelings of uselessness
- Settling outstanding affairs, giving away prized or valuable possessions, or making apology when they are otherwise not expected to dice (every bit an example, this behavior would be typical in a terminal cancer patient but not a healthy young adult)
- Strong feelings of pain, either emotional or physical
- Because oneself burdensome
- Increased use of drugs or alcohol
Additionally, the National Institute for Mental Health includes feeling crushing, and stiff feelings of pain—either emotional or physical—as alarm signs that someone may attempt suicide.[53]
Straight talks [edit]
An effective way to assess suicidal thoughts is to talk with the person direct, to inquire about low, and appraise suicide plans as to how and when it might be attempted.[55] Contrary to popular misconceptions, talking with people near suicide does not constitute the idea in their heads.[55] However, such discussions and questions should be asked with care, concern and compassion.[55] The tactic is to reduce sadness and provide assurance that other people care. The WHO advises to not say everything volition be all right nor make the trouble seem trivial, nor requite false assurances about serious issues.[55] The discussions should be gradual and specifically executed when the person is comfy nigh discussing their feelings. ICARE (Identify the thought, connect with it, Appraise prove for it, Restructure the thought in positive calorie-free, Express or provide room for expressing feelings from the restructured thought) is a model of arroyo used here.[55]
Screening [edit]
The U.South. Surgeon General has suggested that screening to detect those at take a chance of suicide may be one of the most effective means of preventing suicide in children and adolescents.[56] There are diverse screening tools in the form of self-report questionnaires to help identify those at run a risk such every bit the Beck Hopelessness Scale and Is Path Warm?. A number of these self-report questionnaires accept been tested and institute to be constructive for use amongst adolescents and young adults.[57] In that location is all the same a high rate of faux-positive identification and those accounted to exist at risk should ideally have a follow-up clinical interview.[58] The predictive quality of these screening questionnaires has non been conclusively validated and then it is non possible to decide if those identified at risk of suicide will really die by suicide.[59] Asking about or screening for suicide does not create or increase the risk.[60]
In approximately 75 per centum of suicides, the individuals had seen a physician within the yr before their death, including 45 to 66 per centum inside the prior month. Approximately 33 to 41 pct of those who died past suicide had contact with mental health services in the prior year, including twenty pct within the prior month. These studies suggest an increased need for effective screening.[61] [62] [63] [64] [65] Many suicide chance cess measures are not sufficiently validated, and exercise not include all three core suicidality attributes (i.e., suicidal affect, beliefs, and knowledge).[66] A study published by the Academy of New Southward Wales has concluded that asking well-nigh suicidal thoughts cannot exist used as a reliable predictor of suicide risk.[67]
Underlying condition [edit]
The conservative estimate is that x% of individuals with psychiatric disorders may have an undiagnosed medical status causing their symptoms,[68] with some estimates stating that upwards of fifty% may have an undiagnosed medical condition which, if not causing, is exacerbating their psychiatric symptoms.[69] [seventy] Illegal drugs and prescribed medications may also produce psychiatric symptoms.[71] Constructive diagnosis and, if necessary, medical testing, which may include neuroimaging[72] to diagnose and treat whatever such medical conditions or medication side effects, may reduce the risk of suicidal ideation as a result of psychiatric symptoms. Most often including low, which are present in upwards to xc–95% of cases.[73]
Risk factors [edit]
All people tin can be at chance of suicide. Chance factors that contribute to someone feeling suicidal or making a suicide effort may include:
- Depression, other mental disorders, or substance abuse disorder
- Certain medical conditions
- Chronic pain[74]
- A prior suicide attempt
- Family history of a mental disorder or substance abuse
- Family unit history of suicide
- Family violence, including physical or sexual abuse
- Having guns or other firearms in the abode
- Having recently been released from prison or jail
- Being exposed to others' suicidal beliefs, such equally that of family members, peers, or celebrities[54]
- Being male[75]
Legislation [edit]

Suicide and assisted suicide illegal
Suicide legal, assisted suicide illegal
Suicide and assisted suicide legal
Suicide is a crime in some parts of the world.[76] However, while suicide has been decriminalized in many western countries, the act is stigmatized and discouraged. In other contexts, suicide could be utilized equally an farthermost expression of liberty, every bit is exemplified by its usage as an expression of devout dissent towards perceived tyranny or injustice which occurred occasionally in cultures similar aboriginal Rome, medieval Nihon, or today'south Chinese Tibet.
While a person who has died of suicide is across the reach of the law, there can yet be legal consequences in relation to handling of the corpse or the fate of the person's property or family members. The associated matters of assisting a suicide and attempting suicide take likewise been dealt with by the laws of some jurisdictions. Some countries criminalise suicide attempts.
Historically, many laws against suicide and mercy killing accept developed at to the lowest degree in part from religious doctrine: for example, the claim that only God has the right to decide when a person will die.[ citation needed ]
Support organizations [edit]

Sign promoting Samaritans near a payphone about Beachy Head, a major suicide spot in the Britain

A sign at a railroad crossing in the Netherlands promoting a suicide crisis line (113)
Many not-profit organizations exist, such as the American Foundation for Suicide Prevention in the United states, which serve equally crunch hotlines; it has benefited from at to the lowest degree 1 crowd-sourced campaign.[77] The first documented program aimed at preventing suicide was initiated in 1906 in both New York, the National Save-A-Life League, and in London, the Suicide Prevention Department of the Salvation Ground forces.[78]
Suicide prevention interventions autumn into two broad categories: prevention targeted at the level of the individual and prevention targeted at the level of the population.[79] To identify, review, and disseminate information about best practices to accost specific objectives of the National Strategy Best Practices Registry (BPR) was initiated. The Best Practices Registry of Suicide Prevention Resource Eye is a registry of diverse suicide intervention programs maintained past the American Association of Suicide Prevention. The programs are divided, with those in Section I listing bear witness-based programs: interventions which have been subjected to in depth review and for which evidence has demonstrated positive outcomes. Section III programs accept been subjected to review.[80] [81]
If you or someone yous know displays sign or symptoms of suicidal thoughts or actions these prevention organizations are available:
- Befrienders Worldwide
- American Foundation for Suicide Prevention
- Campaign Against Living Miserably
- Crisis Text Line
- International Association for Suicide Prevention
- The Jed Foundation
- National Suicide Prevention Lifeline
- Samaritans
- Suicide Prevention Action Network USA
- The Trevor Project
- Trans Lifeline
Economics [edit]
Although in that location are lasting emotional effects on families due to suicide, the economic effects are contagious. In the United States it is estimated that an episode of suicide results in costs of most $1.3 million.[82] 97 percent of these costs are due to the loss in career productivity from the deceased individual besides every bit the later on-consequence toll on families. Likewise, the remaining 3 percent of the expenses were contributed from medical expenses. Money spending on appropriated interventions is estimated to result in a decrease in economic losses that are 2.5-fold greater than the corporeality spent. Therefore, declaring the need for increased deportment in intervention and prevention to aid uphold individuals, families, and the economy.[82]
See also [edit]
- Advocacy of suicide
- Coping (psychology)
- Coping planning
- Crisis intervention
- Euthanasia
- Gatekeeping (education)
- List of suicide crisis lines
- Living Is For Anybody
- Social skills
- Suicide prevention contract
- World Suicide Prevention Twenty-four hour period
- Suicide awareness
References [edit]
- ^ "Preventing Suicide |Violence Prevention|Injury Heart|CDC". www.cdc.gov. 11 September 2019. Retrieved iii December 2019.
- ^ a b "Suicide|Violence Prevention|Injury Center|CDC". www.cdc.gov. 3 September 2019. Retrieved 3 December 2019.
- ^ a b c d east f Preventing Suicide: A Technical Parcel of Policy, Programs, and Practices (PDF). CDC. 2017. p. 7. Retrieved iii December 2019.
- ^ "Prevention Strategies". world wide web.cdc.gov. 2021-06-04. Retrieved 2022-02-12 .
- ^ "Maine Suicide Prevention Website". Maine.gov. Retrieved 2012-01-15 .
Protective Factors are the positive conditions, personal and social resources that promote resiliency and reduce the potential for youth suicide equally well as other related high-risk behaviors. Merely as suicide risks rise from an interaction between familial, genetic, and environmental factors, so do protective factors.
- ^ Compare: "Suicide prevention definition – Medical Lexicon definitions of popular medical terms easily defined on MedTerms". Medterms.com. 2003-09-16. Retrieved 2012-01-15 .
Suicide should not be viewed solely as a medical or mental health problem, since protective factors such as social support and connectedness announced to play significant roles in the prevention of decease.
- ^ "Means Matter Campaign". Hsph.harvard.edu. Archived from the original on 2012-12-xiv. Retrieved 2012-01-xv .
- ^ "Suicide Prevention Resource Center – Lethal Means". Archived from the original on 2019-05-16. Retrieved 2019-05-08 .
- ^ Yip, Paul SF; Caine, Eric; Yousuf, Saman; Chang, Shu-Sen; Wu, Kevin Chien-Chang; Chen, Ying-Yeh (June 2012). "Means brake for suicide prevention". The Lancet. 379 (9834): 2393–2399. doi:10.1016/S0140-6736(12)60521-2. PMC6191653. PMID 22726520.
- ^ Reisch, T; Steffen, T; Habenstein, A; Tschacher, Westward (September 2013). "Change in suicide rates in Switzerland before and after firearm brake resulting from the 2003 "Regular army XXI" reform". The American Journal of Psychiatry. 170 (9): 977–84. doi:10.1176/appi.ajp.2013.12091256. PMID 23897090.
- ^ Rosenbaum, Janet (2012). "Gun utopias? Firearm access and ownership in Israel and Switzerland". Journal of Public Health Policy. 33 (1): 46–58. doi:x.1057/jphp.2011.56. PMC3267868. PMID 22089893.
- ^ Knipe, Duleeka (2017). "Suicide prevention through means brake: Bear upon of the 2008-2011 pesticide restrictions on suicide in Sri Lanka". PLOS 1. 12 (iii): e0172893. doi:10.1371/journal.pone.0172893. PMC5338785. PMID 28264041.
- ^ Cox, Georgina R; Owens, Christabel; Robinson, Jo; Nicholas, Angela; Lockley, Anne; Williamson, Michelle; Cheung, Yee Tak Derek; Pirkis, Jane (Dec 2013). "Interventions to reduce suicides at suicide hotspots: a systematic review". BMC Public Health. 13 (one): 214. doi:10.1186/1471-2458-thirteen-214. PMC3606606. PMID 23496989.
- ^ "Ways Matter Campaign – Coal Gas Example". Hsph.harvard.edu. Archived from the original on 2012-12-fourteen. Retrieved 2012-01-15 .
- ^ Kreitman, N (Jun 1976). "The Coal Gas Story: United Kingdom suicide rates, 1960–1971". Br J Prev Soc Med. 30 (two): 86–93. doi:10.1136/jech.30.2.86. PMC478945. PMID 953381.
- ^ Okolie, Chukwudi; Forest, Suzanne; Hawton, Keith; Kandalama, Udai; Glendenning, Alexander C; Dennis, Michael; Price, Sian F; Lloyd, Keith; John, Ann (25 February 2020). "Means restriction for the prevention of suicide by jumping". Cochrane Database of Systematic Reviews. 2: CD013543. doi:10.1002/14651858.CD013543. PMC7039710. PMID 32092795.
- ^ "Means Thing – Risk". Hsph.harvard.edu. Archived from the original on 2012-12-13. Retrieved 2012-01-15 .
- ^ "Firearm Access is a Risk Factor for Suicide – Ways Thing Nuts – Means Matter – Harvard School of Public Health". Hsph.harvard.edu. Archived from the original on 2012-12-13. Retrieved 2012-01-xv .
- ^ Vyrostek, Sara B.; Annest, Joseph Fifty.; Ryan, George West. (iii September 2004). "Surveillance for fatal and nonfatal injuries--United States, 2001". Morbidity and Mortality Weekly Report. Surveillance Summaries. 53 (7): ane–57. PMID 15343143.
- ^ Miller, G.; Hemenway, D. (2008). "Guns and Suicide in the Usa". New England Periodical of Medicine. 359 (10): 989–91. doi:ten.1056/NEJMp0805923. PMID 18768940.
- ^ Mann, J. John; Michel, Christina A. (October 2016). "Prevention of Firearm Suicide in the Usa: What Works and What Is Possible". American Periodical of Psychiatry. 173 (10): 969–979. doi:10.1176/appi.ajp.2016.16010069. PMID 27444796.
- ^ Sakinofsky I (June 2007). "The current show base for the clinical intendance of suicidal patients: strengths and weaknesses". Canadian Journal of Psychiatry. 52 (6 Suppl 1): 7S–20S. PMID 17824349.
Other suicide prevention strategies that have been considered are crisis centres and hotlines, method control, and media education... There is minimal research on these strategies. Fifty-fifty though crunch centres and hotlines are used by suicidal youth, information about their impact on suicidal behaviour is lacking.
- ^ Zalsman, Gil; Hawton, Keith; Wasserman, Danuta; van Heeringen, Kees; Arensman, Ella; Sarchiapone, Marco; Carli, Vladimir; Höschl, Cyril; Barzilay, Ran; Balazs, Judit; Purebl, György; Kahn, Jean Pierre; Sáiz, Pilar Alejandra; Lipsicas, Cendrine Bursztein; Bobes, Julio; Cozman, Doina; Hegerl, Ulrich; Zohar, Joseph (July 2016). "Suicide prevention strategies revisited: 10-year systematic review". The Lancet Psychiatry. 3 (seven): 646–659. doi:ten.1016/S2215-0366(16)30030-X. PMID 27289303.
Other approaches that need further investigation include gatekeeper grooming, didactics of physicians, and internet and helpline support.
- ^ General (US), Role of the Surgeon; Prevention (United states), National Action Alliance for Suicide (2012). Introduction. US Department of Health & Human Services (The states). Retrieved 1 May 2020.
- ^ "Recommendations". Reporting on Suicide . Retrieved three December 2019.
- ^ a b Preventing suicide: a resource for media professionals. WHO. 2017. p. viii. hdl:10665/258814.
- ^ Stack, Steven (October 2020). "Media guidelines and suicide: A critical review". Social Science & Medicine. 262: 112690. doi:ten.1016/j.socscimed.2019.112690. PMID 32067758. S2CID 211159266.
- ^ R. F. W. Diekstra. Preventive strategies on suicide.
- ^ a b Smith, Katharine A; Cipriani, Andrea (November 2017). "Lithium and suicide in mood disorders: Updated meta-review of the scientific literature". Bipolar Disorders. 19 (7): 575–586. doi:10.1111/bdi.12543. PMID 28895269. S2CID 39221887.
- ^ Coppen A (2000). "Lithium in unipolar depression and the prevention of suicide". J Clin Psychiatry. 61 Suppl nine: 52–6. PMID 10826662.
- ^ Teicher, Martin H.; Glod, Carol A.; Cole, Jonathan O. (March 1993). "Antidepressant Drugs and the Emergence of Suicidal Tendencies". Drug Safety. viii (three): 186–212. doi:10.2165/00002018-199308030-00002. PMID 8452661. S2CID 36366654.
- ^ Canadian Agency for Drugs Technologies in Health (CADTH) (1 March 2010). "Dialectical Behaviour Therapy in Adolescents for Suicide Prevention: Systematic Review of Clinical-Effectiveness". CADTH Applied science Overviews. i (i): e0104. PMC3411135. PMID 22977392.
- ^ National Constitute of Mental Health: Suicide in the U.S.: Statistics and Prevention [one]
- ^ Stanley B, Brown Grand, Brent DA, et al. (October 2009). "Cognitive-behavioral therapy for suicide prevention (CBT-SP): treatment model, feasibility, and acceptability". J Am Acad Child Adolesc Psychiatry. 48 (10): 1005–13. doi:10.1097/CHI.0b013e3181b5dbfe. PMC2888910. PMID 19730273.
- ^ Kairi Kõlves; Diego De Leo. "Child and youth suicides: Inquiry and Potentials for Prevention" (PDF). Australian Institute for Suicide Research and Prevention. Archived from the original (PDF) on 29 December 2016.
- ^ Riblet, NBV; Shiner, B; Young-Xu, Y; Watts, BV (June 2017). "Strategies to forbid death by suicide: meta-assay of randomised controlled trials". British Periodical of Psychiatry. 210 (6): 396–402. doi:10.1192/bjp.bp.116.187799. PMID 28428338.
- ^ Preventing suicide: a resources for teachers and other school staff. Earth Wellness System. 2000. hdl:10665/66801.
- ^ Stallman, H. K. (2018). "Coping Planning: A patient- and strengths-focused approach to suicide prevention training". Australasian Psychiatry. 26 (2): 141–144. doi:10.1177/1039856217732471. PMID 28967263. S2CID 4527243.
- ^ Stallman, H. M. (2017). "Coming together the needs of patients who take suicidal thoughts presenting to Emergency Departments". Emergency Medicine Australasia. 29 (6): 749. doi:x.1111/1742-6723.12867. PMID 28940744. S2CID 206925361.
- ^ Franklin, JC; Ribeiro, JD; Trick, KR (2016). "Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research". Psychol Bull. 143 (2): 187–232. doi:10.1037/bul0000084. PMID 27841450. S2CID 3941854.
- ^ a b Stallman, H. Yard.; Wilson, C. J. (2018). "Can the mental health of Australians exist improved by dual strategy for promotion and prevention?". Australian and New Zealand Journal of Psychiatry. 52 (half dozen): 602. doi:ten.1177/0004867417752070. PMID 29320871. S2CID 38696679.
- ^ Stallman, H. M.; Ohan, J. L. (2018). "The alignment of law, do and need in suicide prevention". BJPsych Bulletin. 42 (ii): 51–53. doi:10.1192/bjb.2017.three. PMC6001851. PMID 29455707.
- ^ Wegner, Daniel M. (1989). White Bears and Other Unwanted Thoughts: Suppression, Obsession, and the Psychology of Mental Control. Viking Adult. ISBN 978-0670825226
- ^ Engel, 1000. Fifty. (1980). "The clinical application of the biopsychosocial model". American Periodical of Psychiatry. 137 (5): 535–544. doi:10.1176/ajp.137.5.535. PMID 7369396.
- ^ Katsumi, Y.; Dolcos, South. (2018). "Suppress to feel and recall less: Neural correlates of explicit and implicit emotional suppression on perception and retention". Neuropsychologia. 145: 106683. doi:10.1016/j.neuropsychologia.2018.02.010. PMID 29432767. S2CID 3628693.
- ^ Murray, Declan; Devitt, Patrick. "Suicide Hazard Cess Doesn't Piece of work". Scientific American . Retrieved v Apr 2017.
- ^ "National Strategy for Suicide Prevention" (PDF) . Retrieved 2012-01-xv .
- ^ "Suicide Prevention". NIMH. Baronial 2021.
- ^ Shahar, Golan; Bareket, Liad; Rudd, M. David; Joiner, Thomas E. (July 2006). "In severely suicidal young adults, hopelessness, depressive symptoms, and suicidal ideation constitute a single syndrome". Psychological Medicine. 36 (seven): 913–922. doi:10.1017/S0033291706007586. PMID 16650341. S2CID 37342106.
- ^ Linehan et al., 2006
- ^ Stellrecht et al., 2006
- ^ American Academy of Child and Adolescent Psychiatry (April 2001). "Summary of the Exercise Parameters for the Assessment and Treatment of Children and Adolescents With Suicidal Beliefs". Journal of the American University of Kid & Adolescent Psychiatry. 40 (4): 495–499. doi:10.1097/00004583-200104000-00024. PMID 11314578. S2CID 1902038.
- ^ a b "NIMH » Suicide Prevention". world wide web.nimh.nih.gov.
- ^ a b "Suicide Prevention". The National Institute of Mental Health . Retrieved xx November 2019.
- ^ a b c d east "Preventing Suicide – A Resource for Principal Health Care Workers" (PDF), Globe Health Organization, Geneva, 2000, p. 13.
- ^ Office of the Surgeon General:The Surgeon General'southward Call To Activeness To Foreclose Suicide 1999 [2]
- ^ Rory C. O'Connor, Stephen Platt, Jacki Gordon: International Handbook of Suicide Prevention: Research, Policy and Practice, p. 510 [3]
- ^ Rory C. O'Connor, Stephen Platt, Jacki Gordon, International Handbook of Suicide Prevention: Enquiry, Policy and Practice, p.361; Wiley-Blackwell (2011), ISBN 0-470-68384-viii
- ^ Alan F. Schatzberg: The American Psychiatric Publishing textbook of mood disorders, p. 503: American Psychiatric Publishing; (2005) ISBN 1-58562-151-X
- ^ Crawford, MJ; Thana, Fifty; Methuen, C; Ghosh, P; Stanley, SV; Ross, J; Gordon, F; Blair, Yard; Bajaj, P (May 2011). "Affect of screening for gamble of suicide: randomised controlled trial". The British Periodical of Psychiatry. 198 (5): 379–84. doi:x.1192/bjp.bp.110.083592. PMID 21525521.
- ^ Depression and Suicide at eMedicine
- ^ González HM, Vega WA, Williams DR, Tarraf W, West BT, Neighbors HW (January 2010). "Depression Care in the U.s.: Too Little for Too Few". Athenaeum of General Psychiatry. 67 (1): 37–46. doi:10.1001/archgenpsychiatry.2009.168. PMC2887749. PMID 20048221.
- ^ Luoma JB, Martin CE, Pearson JL (June 2002). "Contact with mental health and primary care providers before suicide: a review of the evidence". The American Periodical of Psychiatry. 159 (vi): 909–16. doi:x.1176/appi.ajp.159.6.909. PMC5072576. PMID 12042175.
- ^ Lee HC, Lin HC, Liu TC, Lin SY (June 2008). "Contact of mental and nonmental health care providers prior to suicide in Taiwan: a population-based report". Canadian Journal of Psychiatry. 53 (6): 377–83. doi:10.1177/070674370805300607. PMID 18616858.
- ^ Pirkis J, Burgess P (December 1998). "Suicide and recency of wellness care contacts. A systematic review". The British Journal of Psychiatry. 173 (six): 462–74. doi:x.1192/bjp.173.six.462. PMID 9926074. S2CID 43144463.
- ^ Harris M. M.; Syu J.-J.; Lello O. D.; Chew Y. L. E.; Willcox C. H.; Ho R. C. M. (2015). "The ABC's of suicide risk assessment: Applying a tripartite arroyo to private evaluations". PLOS ONE. 10 (6): e0127442. Bibcode:2015PLoSO..1027442H. doi:10.1371/journal.pone.0127442. PMC4452484. PMID 26030590.
- ^ McHugh, Catherine M.; Corderoy, Amy; Ryan, Christopher James; Hickie, Ian B.; Large, Matthew Michael (March 2019). "Clan between suicidal ideation and suicide: meta-analyses of odds ratios, sensitivity, specificity and positive predictive value". BJPsych Open. five (2): e18. doi:x.1192/bjo.2018.88. PMC6401538. PMID 30702058. Lay summary.
- ^ Hall RC, Popkin MK, Devaul RA, Faillace LA, Stickney SK (November 1978). "Physical disease presenting as psychiatric affliction". Arch. Gen. Psychiatry. 35 (11): 1315–twenty. doi:10.1001/archpsyc.1978.01770350041003. PMID 568461.
- ^ Chuang L., Mental Disorders Secondary to General Medical Weather; Medscape;2011 [4] Archived October 19, 2011, at the Wayback Machine[ needs update ]
- ^ Felker B, Yazel JJ, Brusque D (December 1996). "Bloodshed and medical comorbidity amid psychiatric patients: a review". Psychiatr Serv. 47 (12): 1356–63. doi:x.1176/ps.47.12.1356. PMID 9117475.
- ^ Kamboj MK, Tareen RS (Feb 2011). "Management of nonpsychiatric medical conditions presenting with psychiatric manifestations". Pediatr. Clin. North Am. 58 (1): 219–41, xii. doi:ten.1016/j.pcl.2010.ten.008. PMID 21281858.
- ^ Van Heeringen, Kees; Audenaert, Kurt; Bernagie, Katrien; Vervaet, Myriam; Jacobs, Filip; Otte, Andreas; Dierckx, Rudi (2004). "Functional Brain Imaging of Suicidal Behaviour". Nuclear Medicine in Psychiatry. pp. 475–484. doi:x.1007/978-3-642-18773-5_28. ISBN978-3-642-62287-8.
- ^ Patricia D. Barry, Suzette Farmer; Mental health & mental illness, p. 282, Lippincott Williams & Wilkins;(2002) ISBN 0-7817-3138-0
- ^ Bohnert, Amy South.B.; Ilgen, Ph.D, Mark A. (2019). "Understanding Links amidst Opioid Apply, Overdose, and Suicide". The New England Journal of Medicine. 380 (one): 71–79. doi:x.1056/NEJMra1802148. PMID 30601750.
- ^ "GHO | By category | Suicide charge per unit estimates, age-standardized - Estimates by land". WHO . Retrieved 2021-01-05 .
- ^ Ormerod (ed). Smith and Hogan'south Criminal Law. 13 ed. OUP. 2011. p 583. (This source refers to England before the kickoff of the Suicide Act 1961).
- ^ "GamerGate Leads to Suicide Prevention Charity - The Escapist". www.escapistmagazine.com. Archived from the original on 2017-10-fourteen. Retrieved 2014-09-12 .
- ^ Bertolote, 2004
- ^ Bertolote, Jose (October 2004). "Suicide Prevention: at what level does it work?". World Psychiatry. three (3): 147–151. PMC1414695. PMID 16633479.
- ^ All-time Practices Registry (BPR) For Suicide Prevention Archived 2011-x-31 at the Wayback Machine
- ^
- ^ a b "Costs of Suicide". world wide web.sprc.org . Retrieved 6 March 2018.
Further reading [edit]
- Suicide prevention and assessment handbook, Centre for Addiction and Mental Health, 2011.
- Nancy Boyd-Franklin; Elizabeth N. Cleek; Matt Wofsy; Brian Mundy (2013). "Adventure Assessment and Suicide Prevention". Therapy in the Existent World: Effective Treatments for Challenging Problems. Guilford Press. p. 341. ISBN978-1-4625-1034-iv.
- Van Orden, Kimberly A.; Witte, Tracy One thousand.; Cukrowicz, Kelly C.; Braithwaite, Scott R.; Selby, Edward A.; Joiner, Thomas Eastward. (2010). "The interpersonal theory of suicide". Psychological Review. 117 (two): 575–600. doi:10.1037/a0018697. PMC3130348. PMID 20438238.
External links [edit]
- CDC website on Suicide Prevention
- The Suicide Prevention Resource Center (SPRC) provides prevention back up, training, and resource to assist organizations and individuals to develop suicide prevention programs, interventions and policies, and to accelerate the National Strategy for Suicide Prevention.
- Centre for Suicide Prevention (CSP), Canada
- Suicide Prevention:Effectiveness and Evaluation A 32-page guide from Span United states, the National Center for Injury Prevention and Control, and Education Development Heart, Inc.
- International Clan for Suicide Prevention Organization co-sponsors Earth Suicide Prevention Mean solar day on September 10 every year with the Globe Health Organization (WHO).
- U.South. Surgeon General – Suicide Prevention
- Suicide Risk Assessment Guide – VA Reference Transmission
- Practice Guidelines for Suicide prevention, APA
Source: https://en.wikipedia.org/wiki/Suicide_prevention
0 Response to "Suicide Prevention by Limiting Access to Methods a Review of Theory and Practice"
Post a Comment